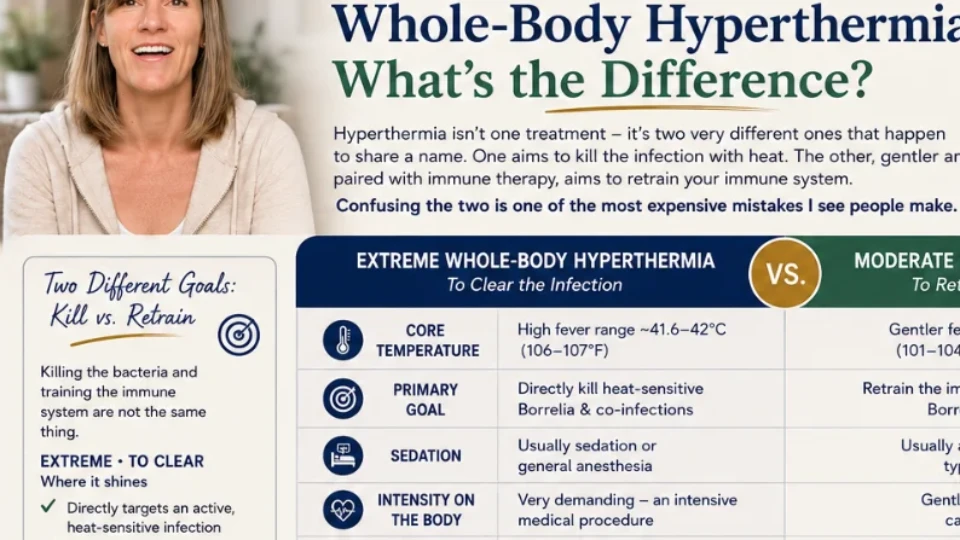
LDN vs. Antibiotics for Lyme: How They Actually Differ
People frame this like a fork in the road — pick one. But that's the wrong mental model. Antibiotics kill the infection. Low-dose naltrexone calms the immune system. They're not two answers to the same question; they're answers to two different questions — and often used together. Here's what each actually does.
"Should I do LDN or antibiotics?" I hear this a lot, and I understand the instinct — when you're overwhelmed, you want a single clear choice. But the honest answer starts by rejecting the premise. Antibiotics and low-dose naltrexone (LDN) aren't competitors doing the same job better or worse. They're doing different jobs. Understanding that difference is what lets you (and your doctor) use them intelligently.
Quick answer
What is the difference between LDN and antibiotics for Lyme?
They do fundamentally different jobs. Antibiotics are antimicrobials that kill or suppress the Borrelia bacteria and co-infections causing Lyme — they attack the infection directly, and for early Lyme they are the standard, often curative treatment. Low-dose naltrexone (LDN) is not an antibiotic and does not kill bacteria; it is an immune-modulating medication used off-label to help calm inflammation and modulate the immune system, which some people find eases pain, fatigue, and other symptoms. In short: antibiotics target the infection, LDN targets the immune response.
Key Takeaways
- It’s not either/or. Antibiotics kill the infection; low-dose naltrexone (LDN) calms the immune system — different jobs.
- Antibiotics target the bacteria and work best early.
- LDN won’t kill Borrelia — it eases pain, fatigue, fog, and an immune system stuck in overdrive.
- They’re often used together, not as competing choices.
- Which you need depends on your situation — usually both, at different points.
Why "either/or" is the wrong question
Lyme is really two problems layered on top of each other: an infection, and what that infection does to your immune system. Early on, the infection is the whole story, and killing it fast usually solves everything. But in longstanding or chronic cases, many people are left with a dysregulated, inflamed immune system that keeps them sick even when the bugs are reduced. Antibiotics speak to the first problem. LDN speaks to the second. Asking "which one?" is like asking whether a house needs a plumber or an electrician — it depends entirely on what's broken.
The side-by-side comparison
| Antibiotics | LDN (Low-Dose Naltrexone) | |
|---|---|---|
| What it is | Antimicrobial medication(s) | Naltrexone at a low dose, used off-label |
| Primary job | Kill / suppress Borrelia & co-infections | Modulate the immune system; calm inflammation |
| Targets the infection? | Yes — directly antimicrobial | No — not antimicrobial |
| Best-established use | Early Lyme — standard of care, often curative | Symptom/immune support, often in chronic cases |
| Typical course | Defined course (early); longer/debated in chronic | Ongoing, daily, low dose |
| Common downsides | Gut/microbiome disruption, yeast, herx, resistance concerns with long use | Generally well tolerated; vivid dreams / sleep changes at first |
| Interactions to flag | Varies by antibiotic | Interacts with opioid medications — needs medical guidance |
| Role | Attacks the cause | Supports the terrain & symptoms |
LDN vs. Antibiotics FAQ
They do different jobs. Antibiotics are antimicrobials that kill or suppress the Lyme bacteria and co-infections — the standard, often curative treatment for early Lyme. LDN is not an antibiotic and kills nothing; it's an immune-modulating medication used off-label to calm inflammation and modulate the immune response. Antibiotics target the infection; LDN targets the immune system.
Often yes — because they do different things, they're frequently complements rather than alternatives: antibiotics for the infection, LDN for the immune response and symptoms. Combining medications is a decision for your prescriber, who can manage interactions and timing (LDN's interaction with opioids especially needs guidance).
No. LDN isn't antimicrobial and doesn't treat an active infection, so it's not a substitute when antimicrobial treatment is needed — especially in early Lyme, where prompt antibiotics are standard and often curative. Think of LDN as supportive immune modulation, not an infection-killer.
LDN is generally well tolerated at low doses; vivid dreams or sleep changes when starting are most common and often settle. Antibiotics can be very effective but may disrupt the gut microbiome, cause digestive upset or yeast overgrowth, and raise resistance concerns with long courses. Herx reactions can occur as bacteria die off. A clinician should monitor either.
At a low dose it briefly, partially blocks opioid receptors, which is thought to raise your own endorphins and modulate immune activity and neuroinflammation. For Lyme the aim isn't to kill bacteria but to calm a dysregulated immune system — which is why some report better pain, mood, sleep, and energy. It's off-label with developing evidence, and should be prescribed and monitored.
References & further reading
- Centers for Disease Control and Prevention (CDC) — Lyme Disease. cdc.gov/lyme
- International Lyme and Associated Diseases Society (ILADS) — evidence-based guidelines and research. ilads.org
- MedlinePlus (U.S. National Library of Medicine, NIH) — Lyme Disease. medlineplus.gov
- Johns Hopkins Lyme Disease Research Center. hopkinslyme.org
General orientation only; specifics vary by individual, antibiotic, and clinical situation. Your prescriber decides what's appropriate.
Antibiotics: killing the infection
Let me be clear about something, because the chronic-Lyme world sometimes gets cynical about antibiotics: for early Lyme, prompt antibiotics are the standard of care and often cure it. If you've just been bitten or have an early infection, this is not the moment to reach for gentle immune support instead — it's the moment for the treatment with the strongest evidence. Antibiotics work by killing or suppressing the bacteria directly.
Where it gets genuinely complicated is chronic or persistent Lyme, where long or repeated antibiotic courses are debated, can be hard on the gut and microbiome, and don't address the immune dysregulation that may be driving ongoing symptoms. That's not an argument against antibiotics — it's an argument for using them for what they're good at, and not expecting them to fix a problem they were never designed to solve.
LDN: calming the immune system
Low-dose naltrexone is the same drug used at much higher doses for other purposes, but at a low dose it does something different: by briefly and partially blocking opioid receptors, it's thought to prompt your body to raise its own endorphins and to modulate immune activity and neuroinflammation. It kills no bacteria. Its job is to help settle an overactive, inflamed system — which is why people using it often report improvements in pain, fatigue, sleep, and mood rather than a sudden "the infection is gone" feeling.
It's used off-label, the research is still developing, and it's not a magic bullet. But it's typically inexpensive, generally well tolerated (vivid dreams when starting are the classic early effect), and appealing precisely because it targets the immune side of the equation that antibiotics leave untouched.
Why they're often used together
Reach for when
- Early Lyme — the evidence-backed first move
- An active infection needs to be reduced
- Under a clinician's defined plan
Considered when
- Inflammation, pain, fatigue persist
- The immune system is dysregulated
- A gentle, ongoing adjunct is wanted
So which do you need?
Reframed properly, the question almost answers itself:
- Early Lyme or an active infection to clear? Antibiotics are the standard, evidence-backed tool — don't delay them for gentler options.
- Cleared or reduced the infection but still inflamed, achy, exhausted? That immune-side picture is where LDN is often considered.
- Both problems at once? That's exactly why they're frequently used together, under one clinician's oversight.
My own bias, from lived experience, is toward treatments that address the immune side of chronic Lyme — because that's the part that kept me and my family sick long after the obvious infection was dealt with. But "bias toward" is not "instead of." The smartest plans I've seen use each tool for the job it's actually good at.
Trying to make sense of your treatment options? Let's talk — free →
Medical disclaimer: This article is for educational purposes only and is not medical advice, diagnosis, or treatment. Antibiotics and low-dose naltrexone are prescription medications; whether and how to use either — including in combination — must be decided and monitored by a qualified clinician who knows your history. Do not start, stop, or change any medication based on this article. Christina Carter is a patient advocate and educator, not a licensed medical provider.