Bullseye Rash but a Negative Lyme Test? Here's What That Really Means
You saw the rash. You did the responsible thing and got tested. And then the result came back negative — while a target-shaped mark stared back at you from your own skin. If you're confused and a little frightened, let me settle one thing right now: that negative test almost certainly does not mean you're in the clear.
Here is the single most important sentence on this page, and I want you to read it twice: a classic bullseye rash is enough to diagnose and treat Lyme — with or without a positive blood test. The rash isn't a clue that needs confirming. In the eyes of essentially every health authority, the rash is the diagnosis.
So if a doctor waved you off because "the test was negative," you are right to feel something is off. Let me walk you through exactly why this happens, why it's so common, and what to do next — calmly and clearly.
Quick answer
Can you have a bullseye rash and still test negative for Lyme?
Yes, and it is common. Standard Lyme testing looks for antibodies, which take about two to six weeks to develop. If you test in the first days or weeks after a bite — which is exactly when the rash appears — your body may not have produced enough antibodies to register, producing a false negative. Major health authorities, including the CDC, note that a classic bullseye rash (erythema migrans) in someone with likely tick exposure is enough to diagnose and treat Lyme without any positive blood test.
Key Takeaways
- A classic bullseye rash is enough to diagnose and treat Lyme — with or without a positive test.
- A negative early test doesn’t clear you. Antibodies take 2–6 weeks; the rash appears sooner.
- The rash outranks the test — in early Lyme it’s the more reliable evidence.
- Don’t let a negative result delay treatment — early treatment works best.
- If your doctor dismisses a clear rash, get a second opinion or a Lyme-literate provider.
Why the test is negative but you still have Lyme
The confusion melts away once you understand what the standard test actually measures. It does not look for the Lyme bacteria. It looks for antibodies — the proteins your immune system builds in response to the bacteria. And antibodies take time to show up.
After a bite, it typically takes two to six weeks for your body to produce enough antibodies to register on a test. But the bullseye rash usually appears within 3 to 30 days — often in the first week or two. See the problem? The rash shows up during the exact window when the antibody test is most likely to be blind.
Rash early, antibodies late
You get bitten. Within days to a couple of weeks, the rash blooms and you rush to get tested. But your immune system hasn't finished building detectable antibodies yet — so the test comes back negative even though the infection is very much underway. This is called a false negative, and in early Lyme it is the rule, not the exception.
It's not just timing, either. A few other things push early tests toward a false negative:
- Early antibiotics. If you were already started on antibiotics, they can blunt your antibody response — hiding an infection that's still present.
- Strain variation. Standard panels don't account for every Borrelia strain, so some real infections slip through.
- An overly strict follow-up test. The Western blot requires a set number of "bands" to count as positive, and can reject genuine cases that don't light up the expected pattern.
This is the same reason so many people with chronic Lyme spend years being told their tests are "normal." The test isn't looking for the thing making you sick — it's looking for your body's reaction to it, and that reaction is an unreliable narrator.
Why the rash outranks the test
Here's the part that should give you back some footing. The bullseye rash — doctors call it erythema migrans — is considered so specific to Lyme that a positive blood test isn't required to diagnose it. The CDC and mainstream guidelines are clear: in someone with likely tick exposure, a classic erythema migrans rash is enough to diagnose Lyme and start treatment. Testing at that stage is often actively discouraged, precisely because it's so likely to be falsely negative and to muddy the water.
The rash is not a symptom waiting for a test to confirm it. In early Lyme, the rash is more reliable than the test.
So when a doctor treats the negative blood test as the final word and overrides a textbook rash, they've got it backwards. The stronger piece of evidence is the one on your skin.
Is it really a bullseye rash?
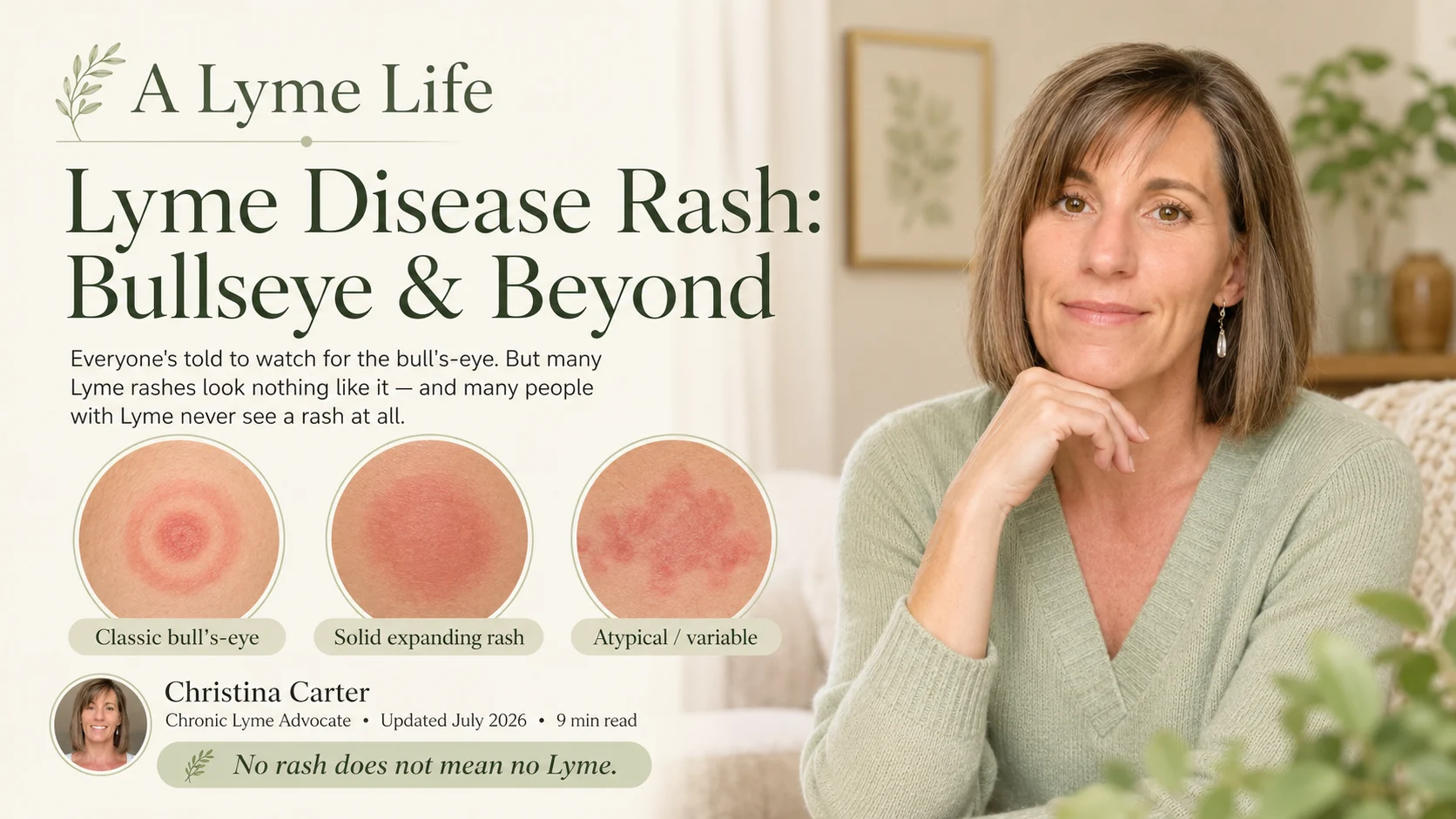
Fair question — and worth a moment, because the "perfect" target ring everyone pictures is only one version. Erythema migrans can look like several things:
- A classic ring within a ring — the storybook bullseye — with clearing in the middle.
- A solid, expanding red or purplish oval with no clearing at all (this is actually very common and often missed).
- A rash that grows over days, often reaching several inches across — expansion over time is a key tell.
- Usually not very itchy or painful, which is part of why people ignore it.
A quick reality check that points toward Lyme rather than a simple bite reaction: an ordinary bug-bite welt tends to appear fast, itch, and fade within a day or two. Erythema migrans tends to appear days after the bite, expand, and stick around. If you can, photograph it with something for scale and note the date — that record is genuinely useful. For the full step-by-step, see what to do the moment you're bitten by a tick.
What to do right now
If you have an expanding bullseye or oval rash and any chance of tick exposure, treat this as time-sensitive. Early Lyme is the stage where treatment works best, so the goal is not to wait around for test numbers to catch up.
- Don't let the negative test delay treatment. Ask your doctor directly about starting treatment based on the rash alone — that's consistent with standard guidance.
- Document everything. Photos of the rash with a date and a size reference, when you think you were bitten, and every symptom (even "minor" ones like fatigue, headache, a stiff neck, or a low fever).
- Save the tick if you still have it. Testing the tick is cheap and fast, and it can tell you what you may have been exposed to. More on that in the tick-bite guide.
- Watch for co-infections. Ticks often carry more than Lyme. If your symptoms are unusual or severe, ask about co-infections like Babesia and Bartonella too.
When (and whether) to retest
If you have a clear bullseye rash, you may not need a test at all to justify treatment — the rash carries the diagnosis. But testing can still play a role, especially if the picture is uncertain or you want confirmation. The key is timing: because antibodies take weeks to build, a test repeated four to six weeks after the bite is far more likely to be accurate than one done in the first few days. This is called convalescent (follow-up) testing, and a rise between an early and later test can be telling.
If you're past the early stage, still symptomatic, and stuck with confusing results, that's where more sensitive specialty testing comes in — I break down the options and the labs Lyme-literate doctors trust in the best Lyme tests guide. And if you want the head-to-head on the two most-recommended labs, see ArminLabs vs. IGeneX.
If your doctor dismisses you
I wish I didn't have to write this section, but I've watched it happen too many times. If a clinician looks at a textbook rash, points at a negative early test, and sends you home with "it's not Lyme," you are allowed to push back — kindly and firmly.
- Ask specifically: "Given the rash and possible exposure, can we treat based on the clinical picture rather than waiting on the antibody test?"
- Ask them to note the rash (and your photos) in your chart.
- If you hit a wall, get a second opinion — urgent care, another primary doctor, or a Lyme-literate doctor (LLMD) who understands early Lyme.
This isn't about being difficult. It's about not letting a known blind spot in a blood test cost you the early-treatment window. Trusting what you can see on your own body is not paranoia — it's good sense. If any of this sounds like the start of a longer story, my piece on being misdiagnosed for years may resonate, and it's exactly the road I want to help you avoid.
Questions to ask your doctor
- The rash looks like erythema migrans — can we treat now rather than waiting on the antibody test?
- Could the negative result be a false negative because it's still early?
- If we do test, should we repeat it in four to six weeks for a more reliable read?
- Should we also consider co-infections given my symptoms?
- What symptoms should prompt me to come back or escalate?
If you're staring at a rash and a negative result and don't know who to trust, I've been exactly where you are — and I'm glad to help you think through your next step and find a doctor who takes early Lyme seriously.
Rash & Negative Test FAQ
Yes, and it's common. Standard tests look for antibodies, which take about two to six weeks to develop — but the rash appears in the first days to weeks, before enough antibodies exist to register. A classic bullseye rash with likely tick exposure is enough to diagnose and treat Lyme without a positive blood test.
No. A negative standard test doesn't rule out Lyme, especially early or after early antibiotics. The test measures your immune response, not the bacteria, and that response can be too early, suppressed, or atypical to detect. Lyme is ultimately a clinical diagnosis.
A classic bullseye rash after possible tick exposure is generally diagnostic on its own, and treatment shouldn't wait on a blood test. Early treatment works best, so don't let a negative early test delay care. If your doctor dismisses a clear rash because of the test, seek a second opinion or a Lyme-literate provider.
References & further reading
- Centers for Disease Control and Prevention (CDC) — Lyme Disease. cdc.gov/lyme
- International Lyme and Associated Diseases Society (ILADS) — evidence-based guidelines and research. ilads.org
- Johns Hopkins Lyme Disease Research Center. hopkinslyme.org
- LymeDisease.org — patient advocacy and education. lymedisease.org
Medical disclaimer: This article is for educational purposes only and reflects personal experience and general research. It is not medical advice, diagnosis, or treatment, and does not replace consultation with a qualified healthcare professional. A rash after a possible tick bite can be time-sensitive — seek prompt care. No laboratory test is perfectly accurate, and early Lyme disease is a clinical diagnosis. Christina Carter is a patient advocate and educator, not a licensed medical provider. Always consult a qualified, Lyme-literate physician about diagnosis and treatment.