MCAS & Lyme: Mast Cell Activation Syndrome, Explained
If you react to everything — foods, smells, heat, supplements — flush red for no reason, and feel like your body is at war with the world, you may be dealing with MCAS. It's one of the most under-recognized pieces of the chronic Lyme puzzle, and once you understand it, a lot of confusing symptoms finally make sense.
MCAS — Mast Cell Activation Syndrome — is one of those conditions that, once you see it, you can't un-see. For so many people fighting chronic Lyme and mold, it's the missing explanation for why they've become intolerant to foods and supplements they used to handle fine, why they flush and itch and swell, why every "gentle" treatment causes a big reaction. Let me walk you through what it actually is, and why it lives so close to Lyme.
Quick answer
What is MCAS (Mast Cell Activation Syndrome)?
MCAS is a condition in which mast cells — immune cells that normally defend the body — become overactive and release their chemical mediators (such as histamine) inappropriately and excessively. Because mast cells sit throughout the body, this causes recurrent symptoms across multiple systems at once: skin (flushing, hives, itching), gut (pain, nausea, diarrhea), airways, heart (palpitations), and brain (fog, anxiety), often triggered by foods, stress, heat, chemicals, or infection. It is a disorder of immune dysregulation rather than a single-organ disease.
Key Takeaways
- MCAS = mast cell activation syndrome — an immune system over-releasing histamine and other chemicals, so you react to foods, smells, heat, and supplements.
- It’s one of the most under-recognized pieces of chronic Lyme.
- The Lyme–mold–MCAS triad is common — the three drive and worsen each other.
- Diagnosis is tricky and usually clinical plus specific lab timing; a knowledgeable doctor helps.
- It’s managed, not “cured,” with triggers, antihistamines/mast-cell stabilizers, and treating the underlying drivers. Your body isn’t broken — it’s overwhelmed.
What is MCAS?
Mast cells are immune cells stationed throughout your body — in your skin, gut, airways, blood vessels, and more. Their job is defense: when they sense a threat, they release a burst of chemical mediators (histamine is the famous one, but there are many) to trigger inflammation and rally the immune response. That's healthy and normal.
In MCAS, that system becomes trigger-happy. The mast cells release their mediators inappropriately and excessively — reacting to things that shouldn't provoke them, and reacting too hard. Because mast cells are everywhere, the result is a bewildering, multi-system pattern of symptoms that seems to touch every part of the body at once. That "everything is connected and nothing makes sense" quality is the signature of MCAS.
MCAS symptoms (face, skin, eyes & flares)
The hallmark of MCAS is multi-system symptoms that come in flares and often track to triggers. Here's how it tends to show up:
Skin & "MCAS face"
Flushing, facial redness and heat, hives, welts, itching, dermatographism (skin that writes when scratched).
Eyes & airways
Itchy, red, watering eyes, puffy lids, nasal congestion, sneezing, throat tightness, air hunger.
Digestive
Nausea, cramping, bloating, diarrhea, reflux, and new food intolerances — especially to high-histamine foods.
Brain & nervous system
Brain fog, anxiety, insomnia, headaches or migraines, lightheadedness, and mood swings during flares.
Heart & circulation
Palpitations, racing heart, blood-pressure swings, and dizziness — overlapping heavily with dysautonomia/POTS.
Whole-body
Fatigue, temperature intolerance (especially heat), and dramatic sensitivity to foods, scents, chemicals, and medications.
Classic triggers include high-histamine foods (aged cheese, fermented foods, leftovers, alcohol, cured meats), heat, stress, strong scents, and even the die-off from treating an infection. The tell-tale sign is reactivity that keeps expanding — your "safe" list of foods and products shrinking over time.
What causes MCAS?
Here's the crucial thing: MCAS is usually secondary — it's driven by something else keeping the immune system on red alert. The most common drivers in the chronic-illness world are:
- Chronic infections — especially Lyme and its co-infections, which keep the immune system chronically activated.
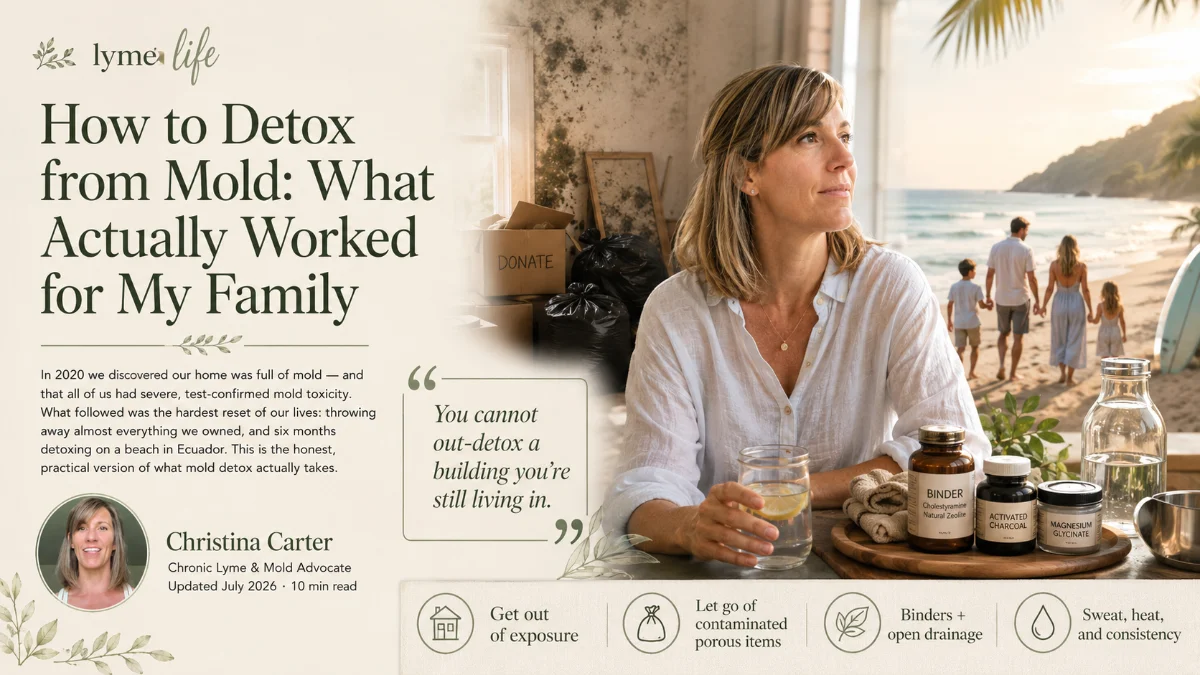
- Mold & mycotoxins — biotoxin exposure is a classic mast-cell provocateur (I lived this; see how to detox from mold).
- Connective tissue disorders — such as Ehlers-Danlos syndrome (EDS), which travels with MCAS and POTS.
- Other chronic inflammatory states and, for some, no single identifiable trigger.
Is MCAS an autoimmune disease?
This is a top question, so let me be precise. MCAS is not classified as a classic autoimmune disease — it isn't the immune system attacking your own tissues (the way lupus or Hashimoto's do). It's better described as a disorder of immune dysregulation: the mast cells are overreactive and misfiring, not self-attacking.
That said, the line is blurry in practice. MCAS frequently overlaps with autoimmune and inflammatory conditions, and it shares the same underlying theme that defines chronic Lyme — an immune system that has lost its proper regulation. That shared root is exactly why these conditions cluster together, and why I think about them as a family rather than as separate silos.
The Lyme–mold–MCAS connection
If you take one thing from this article, make it this. Chronic Lyme, mold illness, and MCAS form a vicious triad — each one inflames the immune system and makes the others worse.
A persistent infection like Lyme keeps your immune system revved, which can tip mast cells into that overreactive MCAS state. That's why MCAS shows up so often in people with chronic Lyme — and why it can be a big reason someone stays sick even after treating the infection. It also travels with dysautonomia and POTS, and it's fed by the same immune dysregulation I write about across this site. Recognizing MCAS is often the key that finally unlocks progress.
How MCAS is diagnosed
MCAS is notoriously hard to pin down, which is part of why so many people go years without a name for what's happening. Broadly, clinicians look for a combination of:
- The clinical pattern — recurrent, multi-system symptoms consistent with mast cell mediator release, affecting two or more body systems.
- Objective markers — laboratory evidence of elevated mast cell mediators (such as serum tryptase measured during a flare, and certain urinary markers like N-methylhistamine or prostaglandins). Timing matters, because levels can normalize between flares.
- Response to treatment — meaningful improvement when mast-cell-targeted approaches are used.
Because testing is finicky and the condition is under-recognized, finding a clinician who actually understands MCAS matters more than any single lab value. A Lyme-literate practitioner is often familiar with it, precisely because of how tightly it links to Lyme and mold.
How MCAS is managed
Management is usually layered, and — I'll be honest — individual. What helps one person can flare another, which is why guidance matters. The common pillars:
- Reduce triggers. Often starting with a low-histamine diet and removing environmental provocateurs (scents, mold exposure, heat extremes).
- Calm the mast cells. Clinicians commonly use H1 and H2 antihistamines and mast-cell-stabilizing approaches; some use natural stabilizers like quercetin or vitamin C as tolerated. These are decisions for your prescriber.
- Support the nervous system. Because stress and a dysregulated nervous system feed mast cell activation, calming that loop (sleep, nervous-system regulation) genuinely helps.
- Treat the root drivers. This is the piece people miss — addressing the underlying Lyme or mold often does more for MCAS than any antihistamine.
Reacting to everything and no one can explain why? Let's talk — free →
MCAS & Lyme FAQ
Mast Cell Activation Syndrome — a condition where mast cells (immune cells found throughout the body) release their chemical mediators like histamine inappropriately and excessively. Because mast cells are everywhere, it causes recurrent, multi-system symptoms (skin, gut, airways, heart, brain) that flare with triggers. It's a disorder of immune dysregulation rather than a single-organ disease.
Not a classic one — it isn't the immune system attacking your own tissues. It's better described as immune dysregulation: overreactive, misfiring mast cells. It does overlap heavily with autoimmune and inflammatory conditions and shares the "loss of immune regulation" theme central to chronic Lyme.
It's usually secondary — driven by something keeping the immune system on alert: chronic infections like Lyme and co-infections, mold and mycotoxins, connective tissue disorders like EDS, and other inflammatory states. For many with chronic Lyme, MCAS is part of a broader immune-dysregulation picture, so addressing root drivers matters as much as calming mast cells.
Multi-system and flaring: flushing and facial redness ("MCAS face"), hives, itching, eye irritation, congestion, food and chemical sensitivities, digestive upset, headaches, brain fog, fatigue, anxiety, lightheadedness, and palpitations. They worsen with triggers like high-histamine foods, heat, stress, alcohol, or strong scents, and often fluctuate dramatically.
Closely. A persistent infection like Lyme keeps the immune system activated, which can push mast cells into an overreactive state — so MCAS is common in chronic Lyme and can keep people sick even after treating the infection. They share the same immune-dysregulation root and often travel with mold illness and dysautonomia. Addressing MCAS can unlock progress in Lyme recovery.
Usually layered: reduce triggers (often a low-histamine diet), calm mast cells (clinicians commonly use H1/H2 antihistamines and stabilizing approaches), support the nervous system, and address root drivers like chronic infection or mold. It's complex and individual, so manage it with a knowledgeable practitioner rather than self-treating.
References & further reading
- Columbia University Irving Medical Center — Lyme & Tick-Borne Diseases Research Center. columbia-lyme.org
- MedlinePlus (U.S. National Library of Medicine, NIH) — Lyme Disease. medlineplus.gov
- International Lyme and Associated Diseases Society (ILADS) — evidence-based guidelines and research. ilads.org
- Centers for Disease Control and Prevention (CDC) — Lyme Disease. cdc.gov/lyme
Medical disclaimer: This article is for educational purposes only and is not medical advice, diagnosis, or treatment. MCAS is a complex condition that must be evaluated and managed by a qualified healthcare professional; diagnostic criteria and treatments vary and are individualized. Do not start, stop, or change any diet or medication based on this article. Christina Carter is a patient advocate and educator, not a licensed medical provider.